- Emergency Ambulance Services
- 8606811111
- 0471-4077777, 0471-7177888
- gro@sutpattom.com
Know Your Food Pipe
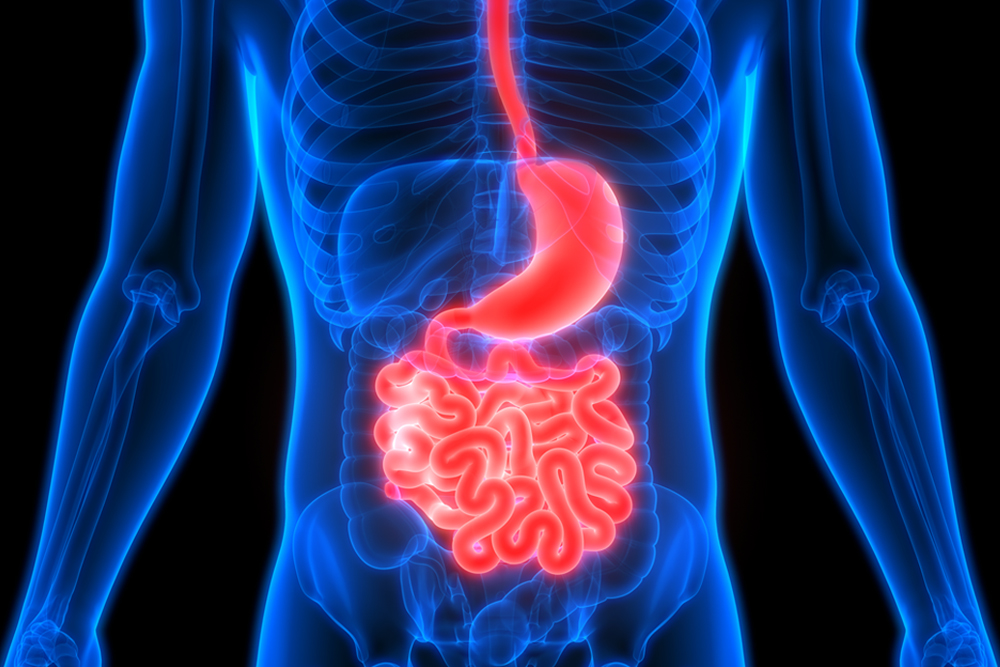
Esophagus (food pipe) is a tubular structure which propels from mouth to the stomach. It is a muscular organ which propels from the mouth in continuous process of successive contraction and relaxation to enter the stomach. The food pipe begins at the level of the neck, runs behind the chest and enters the stomach at a distance of 40 cm from the incisor teeth. The muscularity is formed by a combination of circular and longitudinal muscle layers and is guarded at upper and lower end by the presence of two valves or sphincters which prevents the back flow of food.
The tube is lined internally by mucous layer called squamous epithelium which prevents damage caused by food entering it. Damage or dysfunction of valves allows acidic food from the stomach to reflux and cause damage to the lower part of esophagus causing heart burns. This condition is known as GASTEROESOPHAGEAL REFLUX DISEASE (GERD). It is common in people who smoke, overweight and who consume spicy diet. This condition is confirmed by Endoscopy and an acid probe passed through the entire length of esophagus. If patients are refractory to conservative management by oral medications keyhole surgery is an ideal alternative to provide complete resolution of symptoms by retaining the valvular mechanism.
When the musculature in the lower part of esophagus is weak, destroyed or damaged by congenital or acquired conditions food will be retained in lower part of esophagus causing vomiting. In such patients ACHALASIA CARDIA should be suspected. This condition can be confirmed by passing a pressure probe otherwise known as manometry. Traditionally open surgery was the only option by recently keyhole surgery (hellers myotomy) offers a more painless approach to achalasia cardia.
If the patient complaints of inability to swallow solid food, vomiting, bleeding in the vomitus with loss of weight CANCER in the esophagus should be suspected. It is confirmed by endoscopy and biopsy. Conventional open surgery was the only approach but it was difficult and blind pulling a segment of stomach to the neck for providing a new food pipe after removing the affected esophagus. Usually a large incision in the chest or thorax was needed to mobilize the esophagus which caused excruciating pain and chest complications in postoperative period. The keyhole thoracoscopic approach by camera allows complete visualization and mobilization and avoids such large incision.
Department of SURGICAL GASTEROENTEROLOGY IN SUT HOSPITAL PATTOM is one of the few hospitals in the country to offer keyhole laparoscopic surgery to the entire spectrum of ailments of the esophagus.